We have asked our colleagues in health geography research to tell us about their favourite papers. The following list has been compiled from their suggestions and comments.
Anthony Gatrell, Lancaster University, UK.
'Does the 'average size' of women in the neighbourhood influence a woman's likelihood of body dissatisfaction?'(Lindsay McLaren and Lise Gauvin, 2003)
Health & Place, Vol. 9, Issue 4: p327-335 (Dec 2003)
It is, of course, extremely challenging to select one 'favourite' paper in this research area, since I have found literally dozens that have stimulated and provoked me. In many cases I have thought: 'I wish I'd written that'! But one paper that I have really enjoyed is that by Lindsay McLaren and Lise Gauvin on women's body dissatisfaction in Canada. The premise of the paper was (I quote): "Since body dissatisfaction is linked with and perhaps caused by exposure to images of thin women , it is reasonable to hypothesise that in an environment where women actually are thinner, body dissatisfaction will be more likely." Using a telephone survey of 884 women the authors found that, while body dissatisfaction was related to the individual's body mass index, it was also linked to the average BMI of women living in the same neighbourhood. Simply, a woman was more likely to feel dissatisfied with her body if she was 'surrounded by' women who were thinner than her.
I like this paper because it is very geographical: place, or 'context' matters. So much of what now appears in geography journals seems to have little or nothing to say about location, or place, or space. In this study, where you live makes a difference to your life. To have evidence that the way you feel about yourself depends in part on how you see (literally) others living nearby is rather powerful. Of course, as the authors recognise, there are all sorts of difficulties in conceptualising 'neighbourhoods', and much of our self-esteem depends upon our responses to other images that are not place-specific. Nonetheless, among other studies that bring out the importance of spatial context, this is a winning number, so much so that I was keen to include it in the second edition of Gatrell & Elliott (Geographies of Health, Wiley, 2009).
Graham Moon, University of Southampton, UK.
'Area, class and health: Should we be focusing on places or people?'(Sally Macintyre, Sheila Maciver and Anne Sooman, 1993)
Link Unavailable
'From distributions of deviance to definitions of difference: past and future mental health geographies'(Jennifer Wolch and Chris Philo, 2000)
Health & Place, Vol 6, Issue 2: p137-158 (Sept 2000)
I've had a long think about this and I really don't have one single favourite. My thoughts included Wil Gesler's Epidauros paper in SSM which really set the therapeutic landscapes theme going, Robin Kearns' paper on Hokianga in the same outlet (a favourite because I know the place well), Paul Knox on inequalities in access to GPs in Scottish cities years ago in EPA but a paper of its time and one that was quite influential in getting me into health geography, most papers by Subramanian as he writes so well and exemplifies what you can do with multilevel models... The list goes on. If really pressed my top two are Sally Macintyre, Sheila Maciver and Anne Sooman (Ellaway) on area, class and health in Journal of Social Policy - a classic, starting off the composition and context debate - and Jennifer Wolch and Chris Philo's paper on past and future mental health geographies in Health and Place (12 years on and still a point of reference, generous, comprehensive and even handed).
Kelvyn Jones, University of Bristol, UK.
'Hybridising Alternative Models of an Epidemic Diffusion Process' (Peter Hagget, 1976)
Economic Geography, Vol. 52, No. 2, p.136-146 (Apr 1976)

I have chosen it because it analyses space time data not merely as a technical exercise, but in a way that engages the geographical imagination. I will try and explain. The graphs below show 2 distinct patterns a) is for one week and b) is for another. The circles are places proportional to the size of the population, and are coloured black if there are measles cases in that week, left blank otherwise.
Graphs c) and d) show these places connected in 'neighbourhood space' so that places near each other are joined. It is clear that the left-hand graph of c) is strongly patterned - there are many 'Black - Black' joins, and 'White - White joins', but no 'Black - White' joins. This is strong positive spatial autocorrelation - there is a clear patterning in neighbourhood space. But if you look at the right-side (d), in this week there is not strong patterning with both same colour and different colour joins. The next set of graphs looks at the two weeks when places are joined in hierarchical space - with the biggest place connected to the next biggest place and so on. Now it is the right-hand graph of f) that has the strong patterning when viewed in hierarchical space, but the autocorrelation is less strong for e) with this form of connectivity.
In the paper Peter Hagget uses seven different join systems reflecting different types of connectivity, and therefore potentially seven different types of spatial spread.
G1: local contagion assuming a spread only between contiguous districts;
G2: wave contagion assuming spread by shortest path from Plymouth;
G3: regional contagion assuming spread occurs within two regional subsystems based on east and west Cornwall;
G4: urban and rural hierarchical spread within seperate sets of urban and rural districts;
G5: hierarchical assuming spread down the population-size hierarchy;
G6: hierarchical assuming spread down the population-density hierarchy;
G7: journey-to-work contagion assuming spatial spread from urban centres to surrounding riral areas;
For each of the sets of joins (or spatial weights) as they are known, he calculates a measure of autocorrelation - the degree of map pattern for different weeks over the course of an epidemic of measles in Cornwall.
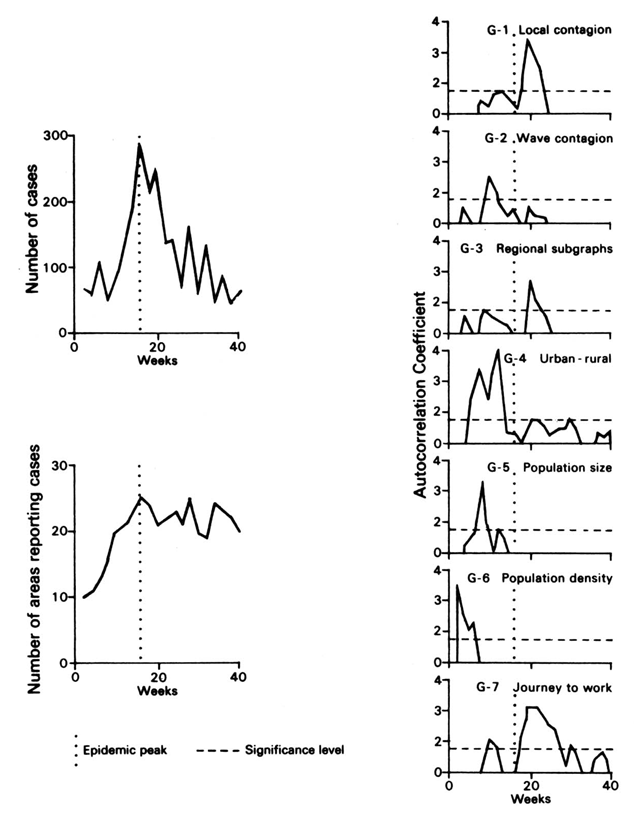 Early in the epidemic, before it has reached the peak, there is significant patterning for joins based on Population density and Population size suggesting that the spread is hierarchical; it trickles down the population hierarchy. However, later on the strongest patterns are for joins based on Local contagion and Journey to work, suggesting that the spread is more localised and based on distance. Different spatial processes are important at different stages of an epidemic's development. It is no good immunising locally at the beginning of an outbreak as it is likely to have jumped to the larger towns and cities in the region.
Early in the epidemic, before it has reached the peak, there is significant patterning for joins based on Population density and Population size suggesting that the spread is hierarchical; it trickles down the population hierarchy. However, later on the strongest patterns are for joins based on Local contagion and Journey to work, suggesting that the spread is more localised and based on distance. Different spatial processes are important at different stages of an epidemic's development. It is no good immunising locally at the beginning of an outbreak as it is likely to have jumped to the larger towns and cities in the region.
This would have been a great deal of work in the early 1970's given available computing power. It is a great pity that much of what has followed in using such spatial models has been very unthinking in only using one measure of spatial connectivity and not considering the nature of the process involved.
If you want to read more;
Haggett, P (2004) The Geographical Structure of Epidemics, Oxford University Press.

{kind=link}